Denis Oriot, Guillaume Alinier, Zineb Messarat-Haddouche, Hervé Thomazeau, Laetitia May-Michelangeli, Marie-Christine Moll, Jean-Claude Granry (Author)
Simulation can be used in healthcare education to provide learners with the opportunity to develop the knowledge and skills needed to manage complex situations and provide patient care, however one aspect easily overlooked and which has many ramifications, is that of ethical practice.
Simulation-based education is a moral and ethical imperative. “Never the first time on the patient!” is displayed at the entrance of some clinical simulation centres, but the rest of the ethical obligations, besides the professional code of ethics, are either not mentioned or only sporadically.
By using an interpretive framework based upon the 4 bioethics principles used for patients (autonomy, beneficence, nonmaleficence, and distributive justice), we propose, as a conceptual framework, an analysis on the stakeholders of simulation-based education (SBE) - educators, learners, and simulated participants - to broaden and explore in depth the conventional views of ethics in simulation. This article also discusses specific features in simulation which sometimes pose an ethical dilemma such as facing simulated death, breaking bad news, research, the use of biological tissue, teaching ethics, and computer simulation.
This proposal to explore ethics in healthcare simulation is intended to stimulate reflection rather than serve as a model seeking external validation.
Foreword
Before embarking on exploring ethics in healthcare simulation as a conceptual framework, we believe it is important to clarify the relationship between a practice, its ethical aspects, and its legal aspects. The relationship between biomedical practice, ethics, and legislation is closely tied to a society’s historical, cultural, political, and religious context [1, 2]. More specifically, the relationship between ethics and the law regarding a given action evolves according to dynamics shaped by this context. Two examples related to simulation illustrate this point:
1. In France, donating a body to science has been legal since 1953, provided there is prior consent from the donor and that it is done with due respect for the body [3]. In 2019, a scandal was revealed by the press at an anatomy laboratory at Paris-Descartes University involving the discovery of inappropriately managed dismembered bodies and scattered anatomical parts [4]. Yet it was legal and must have been practiced in other laboratories for years. The fact that there were also illegal practices (poor hygiene, removal of jewelry from corpses) triggered an investigation and revealed a set of practices that had become unethical. This, in addition to disciplinary action against an individual, was deemed unethical (in light of the evolving concept of due respect for the body since 1953) and prompted the government to put a new law in place to better regulate this practice [5]. Thus, French law is the product of what occurs within the context of French society and may or may not correspond to practices in other countries. It is neither transferable nor generalizable. It may inspire other communities to amend their legislation in accordance with their historical, cultural, political, and religious contexts. In this case, the practice of donating one’s body to science was originally legal and ethical; however, due to illegal abuses, it aroused appropriately founded concerns and came to be viewed as unethical in its current form, prompting lawmakers to strengthen the law to align with bioethical principles as perceived by the French public in 2022 [6].
2. As of today, in France as elsewhere, the use of Artificial Intelligence (AI) is legal (or rather, not illegal) and ethical in simulation. However, certain developments in AI may be viewed as risks that challenge bioethical principles. In such situations, a country’s legislation might need to change to legally regulate the use of AI, for example, if there is a potential harm to individuals. In other countries, this use could continue unhindered. Finally, for certain communities, although legal, the use of AI should comply with a code of ethics established by one or more medical societies. We thus see the importance of the sociological context regarding the tensions between legislation and ethics that may arise over time, and the dynamics that enable their resolution. For example, would it be ethical to have an AI entity conduct a debriefing of a healthcare professional following a simulation-based activity in order to determine whether they can return to work after an extended sick leave? For now, this is neither mandatory nor illegal, but is it ethical? [7].
Consequently, the approach we present here is closely tied to the sociological context of our country of origin and, therefore, to the evolution of its legislation. This is inevitable in any human community.
Introduction
The rapid and universal deployment of simulation in healthcare for educational or system testing or redesign purposes raises the question of its limits. Technological limits seem ephemeral, falling one after the other as years go by. However, simulation in healthcare, like any human activity, has ethical limits that codify and modulate the use of these technological advances.
Here we propose a conceptual framework that allows us to broaden and explore in depth the conventional view of ethics in simulation, which is tied to the principle of beneficence toward the patient (“never the first time on the patient”). In fact, the rest of the ethical obligations besides the professional code of ethics, are either not mentioned or are mentioned only sporadically.
Because simulation in healthcare education is an activity aiming to improve patient care, we have chosen to use the “bioethical principles” tool – usually reserved to patients or research participants – to describe these limits and apply them to activities concerning people who are upstream or downstream of the use of simulation as an educational approach, taking into account the different people who may use it, and highlighting the conflicts that may exist between certain bioethical principles in particular situations. Therefore, the objective of this article is to provide a broader and more detailed perspective on ethics in simulation using the framework provided by bioethical principles. It includes not only patients but also all stakeholders (educators, learners, and simulated participants) and to examine several specific simulation situations. This proposal to explore ethics through healthcare simulation is intended to stimulate reflection rather than serve as a model seeking external validation outside of its sociological context.
This article is based on the simulation in healthcare good practice guide published in March 2024 by the French National Healthcare Authority [8].
Simulation-based education is an ethical and moral imperative
The benefits of simulation-based learning in healthcare have been demonstrated [9, 10], and like any human activity, it has both ethical and professional requirements and limits. The four principles of bioethics are autonomy, beneficence, non-maleficence, and distributive justice [11]. Simulation in healthcare education is an ethical and moral imperative for healthcare professionals and trainees with respects to their patients, as Ziv et al. put it over twenty years ago [12]. Simulation therefore begins with an important moral commitment: ‘’We must do the best we can to keep patients safe while training the next generation of clinicians and retraining current clinicians so that they are kept up to date. If we can introduce clinicians to patients when these clinicians have more “experience” with quasi-patients of a wide variety, we lessen the chances that vulnerable patients will be harmed. Ethics is not an add-on to simulation; an ethical claim drives the practices of simulation themselves’’ [13].
Furthermore, simulation has an epistemic role in that it can transform theoretical knowledge into practical know-how, enabling the universal application of international recommendations for patient wellbeing [14, 15]. Simulation users as educators must therefore endorse a professional ethics and have the responsibility of training all healthcare professionals at the highest level of performance possible.
Ethics and simulation-based education
The principles of bioethics can also be extended to everything patient related. If the care provided to patients appears to be the primary concern - the ethics of simulation-based education (SBE) for the patient - so too is the learning of the healthcare professionals who will deliver this care. Indeed, better learning is the key to better care [16]. This objective can also include the ethics of those involved in the educational process. In this way, we can define the ethical aim and content of the various bioethical principles applied to these people and which we have summarised in Table 1.
For patients
The ethical aim for patients is that simulation should help them receive the best possible care according to current evidenced-based practice.
Autonomy, the ability to decide for oneself, was reinforced by the French Law of March 4, 2002 [17]. It is essentially based on the principle of information and consent. In the domain of healthcare education, it can refer to informing patients that the training of healthcare professionals involves the use of simulation. This can be done through disclosure in the patients’ welcome booklet or on information boards, but also orally before a procedure is performed, for example. It has been reported that patients preferred to have a procedure performed by a simulation-trained professional rather than by a professional who has not been trained using simulation [18]. This also includes information on the fact that procedures performed by a junior simulation-trained clinician will be supervised by a more senior clinician, with the inevitable patient right of refusal without prejudice. Another aspect relates to the commercial independence of prescriptions (medical devices and drugs) made for the patient. In the case of in-situ simulation in a real clinical setting, it is imperative to inform patients on the unit that there are two teams: a care team and a simulation training team. The latter may cause some noise and temporary inconvenience, but it should never to the detriment of patient care. Once the patient has been given clear, fair information in a language they can understand, written consent for the treatment should be obtained.
The principle of beneficence means looking for elements of the simulation that are intended to benefit the patient. The Kirkpatrick pyramid [19] can be used to classify them into levels.
Simulation-based training aims to benefit the patient by improving the performance level of healthcare professionals (Kirkpatrick level 2 = K2), changing professional practices and increasing compliance with recommendations (K3). Simulation benefits patients by reducing morbidity (complications, worsening, etc.) and mortality in the rare studies that have reached K4 [20, 21]. Simulation has also been shown to reduce healthcare costs [20, 22], which can be considered as level 5 of the Kirkpatrick's pyramid (K5). The arguments are so numerous that this led to the saying “Never the first time on the patient” being displayed at the entrance of some clinical simulation centres [23].
The principle of non-maleficence corresponds to tracking down conflicts of interest that would lead to harm for the patient. For example, excessive development of in-situ simulation at the expense of clinical timetables or human resources for patient care would be a case of maleficence. Similarly, the risk of mixing of simulated drugs and medical devices with those dedicated to real patients in a clinical unit where in-situ simulation is taking place, would also be a case of maleficence [24]. The same would apply if a patient room used for in-situ simulation was not cleaned before a patient was admitted. There could be unfortunate consequences in terms of iatrogenic and nosocomial infections.
Applying the principle of distributive justice means, on the one hand, ensuring that all patients can benefit from healthcare professionals trained using SBE, and, on the other hand, that the care delivered by trained staff is provided to all patients, regardless of resources, religion, opinion, ethnicity, age or gender... irrespective of the type of service, the status of the staff and their working hours (day or night shift), 24 hours a day, 7 days per week.
For educators
Immersive scenario-based simulation probably provides the best possible learning experience in the field of health to learners so that they develop better skills, provide more humanistic care, avoid errors and adverse events, and minimize their consequences, and thus make medical practice safer [25]. As such, educators should have for ethical aim to foster the use of SBE at every opportunity.
Autonomy. A first obstacle to this freedom would be resistance to the ''simulation'' concept by decision-maker (hospitals, universities, professional and accreditation bodies...). In this respect, it is interesting to go back to the beginnings of simulation in aeronautics, which encountered this same obstacle. As McLoed said in the late 1960s: ‘’I expressed my growing concern for the future of mankind and my intention of applying the technology of simulation to help alleviate the problems of society. It hasn't been easy. Among other things I have felt grave concern over the lack of acceptance of the results of modelling and simulation. In a time of increasing complexity of life, when decision-makers need all the help they can get, the very powerful tool of modelling is sometimes not used, or is misused, or the results of modelling, once obtained, are not acted upon’’ [26]. These words are still relevant today in the world of healthcare. This ethical obstacle has largely been overcome by the inclusion of SBE in initial and continuing training programmes, and other governmental or professional initiatives [27].
Secondly, autonomy could correspond to the freedom to initiate SBE programmes without being dependent on commercial companies. However, freedom of choice in the acquisition of simulation equipment depends on sources of funding, and therefore on institutional, regional, and national political powers to supply these resources. Otherwise, these same institutions must guarantee and enforce ethical rules with regards to companies. These rules are now well established and guarantee the educators’ autonomy in the practice of healthcare simulation. Another problem that can hamper the freedom of the simulation educator is the growing competition between multiple companies, making this choice inevitably subject to commercial pressures (discounts on the purchase of several models, addition of complimentary devices in the event of an expensive purchase...). Paradoxically, the absence of freedom of choice linked to a governmental decision can make it possible to free oneself from financial influence struggles. An example is the recent purchase by each medical school in France of the simulation models required for Objective Structured Clinical Examinations according to a list prescribed by a national steering committee. This underscores the importance of drafting and disseminating recommendations on pedagogical efficiency, which should prevail over any costly investments in the field of healthcare SBE.
One might think that the beneficence for the educator would be the ease with which they could deliver courses without institutional or financial obstacles, and that these courses could clearly benefit learners. This largely depends on the “simulation culture” of a country or region, and on the way in which legislative texts related to the use of SBE for healthcare professionals are applied, as well as on the acceptance and integration of simulation education concepts and tools by those involved.
Non-maleficence. All too often, the use of simulation as a learning approach in the healthcare professions involves resolving professional practice conflicts. The primary conflict in many countries, is the educator's personal time dedicated to SBE when they have a full-time clinical role. This time is still often the educator's personal time, not identified or accounted for by the employer. Such personal time commitment initially made it possible, and is still an enabler to launch SBE activities in many institutions, but under no circumstances can it be made permanent, at the risk of undermining motivation. The second conflict concerns in-situ simulation. This often takes place in emergency care units and must be balanced against the care of real patients [24]. Limited staff resources hamper the development of in-situ simulation, which can only take place when the patient flow remains reasonable.
Applying the principle of distributive justice to simulation educators means talking about access to SBE for educators in relation to their own training. This is largely dependent on country, culture, and mentality. Two examples illustrate this point. The first is the assistance in equipment and training provided by volunteer international educators in 2013 from the International Paediatric Simulation Society to the only paediatrician in Malawi to improve infant care in the country [28]. The second example is the beneficial action of the programme “Helping Babies Breathe” carried out in 2016 by the American Academy of Paediatrics, supported by the United Nations High Commissioner for Refugees, and sponsored by the Laerdal Foundation in Ghana, Rwanda, Indonesia, and Nepal. This involved the supply of low-cost newborn manikins with a training programme, teaching material, training of trainers, evaluators for initial and remote monitoring over several years, resulting in a significant reduction in neonatal mortality [29]. Another issue in some countries is the impossibility for healthcare professionals to have access to anatomical subjects for SBE purposes due to religious barriers. For example, Libyan surgeons have twice come to France to train on the SimLife model [30]. An alternative approach is the use of synthetic or digital simulation tools as they allow for the rapid dissemination of SBE, requiring only a power outlet and internet access.
Other principles
For educators, it is important to add two other aspects of ethics that cannot be included in bioethics principles: professional ethics and the ethics of responsibility.
Professional ethics refers to procedural ethics including all the rules of good SBE practice [31], while keeping learners safe, preventing errors and facilitating learning, as described as imperatives in the Society of Simulation in Healthcare's Code of Ethics [13, 32]. Furthermore, SBE also involves training in the practice of debriefing so that it is relevant and non-offensive [33]. This benevolence towards learners is part of the rules of healthcare simulation and attempts to mirror the principle of beneficence that should guide healthcare professionals towards doing their best for their patients. It is an essential professional ethics principle, and this notion comes close to the ethics of virtue by “doing good” for the patient and for the learner [34], but also anchoring this ability in the absolute necessity of evaluating the performance of learners' actions and behaviours.
The idea of an ethic of responsibility for the educator is that they must do everything possible to obtain results corresponding to the K2, K3, and even K4 levels of Kirkpatrick's pyramid [35, 36]. The ethical importance of evaluation in SBE can be seen here, as it is the only way to demonstrate progress in learning and performance.
For learners
The ethical aim for learners in a simulation programme is to benefit from the best possible education to develop their knowledge and competence to improve patient care.
Autonomy. In initial training, like in continuing professional development, the validation of SBE has almost become an obligation [37]. Learners must be briefed concerning any SBE activity they get involved in and give their consent [38, 39]. Inappropriate briefing or consent increases the risk of a difficult debriefing which could impact the learning process [40, 41].
Information within the briefing must include various elements:
- Educators’ compliance with the Simulation Code of Ethics [32].
- Context of the activity (pre-briefing and orientation): Review of prerequisite learning, presenting ground rules (confidentiality, benevolence, respect, neutrality, mutual trust), and type of activity (scheduled/unannounced, summative/formative) [36]. It is also important to help learners familiarise with the environment (centre or in-situ, peri-situ) and the medical and simulation equipment [42]. If there is a formative assessment of performance during the scenario, it is only for guiding the debriefing and it will not be transmitted to anyone in the clinical setting.
- Briefing: Providing an introduction to the scenario; explaining that it may include specific critical procedures with a causal link to the survival of the “patient” [42].
- Limitations of the simulation experience: Possible differences from practice in a clinical unit and potential technological issues with the manikin [43], up to the point where a scenario may have to continue in a verbal form.
- Need for engagement – with the ‘’as if’’ concept so learners suspend disbelief about aspects that lack realism [43-45]. Suspension of disbelief becomes the core of the efficiency of SBE and is agreed upon as part of a fiction contract established with the learners [46].
- Awakening to the knowledge of possible “intruders”. Unexpected external events may be planned in the scenario to approximate reality such as the visit of angry relatives, voluntary malfunction of a device, unavoidable death of the manikin, etc. In this case, the information is limited to: “You are required to deal with the present case as you would in real life”. Other elements independent of the scenario's story must also be given to learners, so that they can freely accept the simulation without feeling prejudiced [47].
- Use of personal data: give full details of how any video recording of the activity or learners' computerized performance data collected by any type of sensors will be used.
- Independence from any commercial interest: There should be no passive commercial seeding of learners, fraudulent reuse of digital data (mailing lists...), devices, healthcare services in all their forms, direct or indirect (48-50).
- Assurance of the ethical aspect of the simulation model: for a simulated patient: acceptance of the role, irrespective of their age (51); for the use of cadavers: compliance with the rules governing the donation of the body to science (5); for an animal anatomical part: compliance with ethical rules related to animals (52, 53).
For learners, the principle of beneficence amounts to asserting that SBE provides a benefit, and in the case of normative evaluation, training validation or recertification (54). This benefit is based on the rules of SBE, especially benevolence.
- The scenario should be adapted to the learners' level so as not to set them up for failure but just to challenge them enough so they operate at the edge of their comfort zone whereby they may be expected to make mistakes without being completely overwhelmed (14, 55).
- The realism, which corresponds to the fidelity of the “simulation” experience as perceived by the learners (environment, model, and scenario), should match the clinical reality required to achieve the activity’s learning objectives whilst also providing learner satisfaction (K1) (36, 43). This may also be linked to the possibility of interacting with the model: simulated patient, manikin, Virtual Reality simulator, cadaver, etc. (56-58). These elements (environment, model, scenario) combined with psychological fidelity (contextualization of the scenario and realistic and immersive engagement of the learners in the activity), constitute the 4 elements of simulation fidelity, which corresponds to the highest level of realism (43). This guarantees that learners are exposed to a valid SBE experience.
- The increase in knowledge, know-how, interpersonal skills, as well as self-confidence and a sense of personal efficacy, corresponding to level K2 (36).
- The debriefing should be of quality, respectful, non-offensive, and relevant. This is dependent on the training of the educators so they develop optimal debriefing skills (59).
Respecting the principle of non-maleficence means avoiding any harm to learners or ensuring that any potential harm is associated with a positive benefit/risk ratio. This is about not “tricking” learners with bad intentions, nor purposefully provoking negative emotions. The feeling of being deceived can come from the scenario itself, from simulated participants, or from an intentional equipment malfunction [43, 47]. Negative emotions can also be generated by the provoked and unavoidable death of the “patient” [60]. It is important to realise that deception is often purposefully incorporated into scenarios to enhance their authenticity, and hence it is no related to
non-maleficence but benevolence [43]. If the simulation is multi-professional, and even more so in-situ, then a tension arises between the “good for the team, the unit, the institution” (imagining all possible cases, even the most difficult) and the “good for the learner” (avoiding the feeling of deception). It also raises a dilemma between the scenario's loss of authenticity, which threatens the principle of beneficence, and the learners’ loss of psychological safety, which threatens the principle of non-maleficence [61].
It is on this basis that a controversy has arisen in the world of SBE about whether or not it is possible to deceive learners for their own good. The key lies in the quality of upstream information, which is the learners’ preparation in the form the pre-briefing and associated learning contract [43].
The principle of distributive justice applied to the learner is that all learners should benefit from SBE. This requires well trained simulation educators, sufficient training space, and good administrative and technical support and processes. All these elements ensure the reproducibility and accessibility of SBE to all learners.
For simulated participants
The ethical aim for a simulated (or standardized) participant or patient (SP) is to increase the realism of a scenario. Learners are still immersed in a controlled environment within which they can make mistakes and develop technical and communication skills without this being harmful to the patient [43].
The principle of autonomy for the SP corresponds to the freedom to choose to be involved in a scenario depending on the level of physical exposure required, the type of physical assessment or procedures to be performed on them, and the type and tone scenario script language [62]. This is similar to an actor’s right to accept or not a role and its associated script for a movie. Prior information must be as exhaustive as possible, specifying the number of scenarios enacted over a set duration, the break times, and so on. It is also important to provide a framework that includes role portrayal training, image rights, and training to evaluate learners’ performance or providing feedback. Two examples illustrate the possible limits of the role of SPs: Their use to teach pelvic examination [63] or to receive repeatedly a diagnosis with a poor prognosis [64].
Beneficence. Simulated patients need to work in good conditions, including a space where they can get changed, “get in” and “get out” of character, and wait between scenarios [62, 65].
The benefits of participating in SBE for SPs can be of various kinds: 1/ Participation in improving the skills of healthcare professionals, particularly for expert patients; 2/ Personal development in another field of theatrical art for actors; 3/ Financial benefits through remuneration for preparation time, simulation-based activity with learners, and travel expenses [65, 66].
Respecting the principle of non-maleficence corresponds to avoiding the simulated patient's insecurity. This is essentially psychological but also physical insecurity in relation to body parts exposure. This means ensuring the psychological safety and mental wellbeing of the SPs by taking care of not awakening negative prior experiences, evaluating the impact of the frequency of training situations on the SPs’ psyche (e.g., the consequences of being diagnosed with cancer several times a day/week), and debriefing the SPs regularly about their role and experience and offering the support of a psychologist if needed [65, 67].
Distributive justice would correspond to the national and international availability and use of SPs for the training of healthcare professionals in SBE programmes.
Other principles:
There is a professional ethical principle whereby the SPs must accept to take part in training sessions to learn how to act as per the patient they need to impersonate and how to provide feedback to learners or complete evaluation forms about their performance. They need to accept receiving feedback on their own acting performance. They must respect a certain number of points linked to SBE [62]. These include adhering to the principles of simulation including confidentiality (especially for in-situ simulation) and benevolence.
Special features
Ethics and disclosure of bad news
When it comes to breaking bad news in simulation, the psychological safety of learners and SPs cannot be ignored. It is part of professional ethics, without which learning becomes random or dangerous. Indeed, the disclosure of bad news refers to the emotions expressed by SPs that can provoke a psychological distress in relation to an event already experienced by learners [68]. This can raise ethical issues and cause trauma for learners [69]. For this reason, making sure at an earlier stage that this type of simulation does not disturb the learner and that the verbal and behavioural expressions of the SPs are not too destabilizing for a beginner learner helps to ensure their
psychological safety.
Such assessment can be based on the SPIKES method (Setting, Perception, Invitation, Knowledge, Empathy, Strategy, and Summary) [70] or its French translations – EPICES (Environnement, Perception, Invitation, Connaissances, Empathie, Stratégie et Synthèse) [71].
Ethics and death in simulation
After several decades of simulation during which educators advocated against allowing the simulator to die unless death was part of the learning objectives [72], this practice has been called into question.
There is a profound discrepancy between cardiopulmonary resuscitation (CPR) management in simulation compared to real life: it is shorter and a lot less sad [73]. The risk is therefore a loss of “fidelity” of the scenario and thus a threat to the principle of beneficence as the learning experience no longer fully exposes learners to the reality of clinical practice.
It has also been reported that presenting scenarios with a systematic death of the manikin leads to an increase in anxiety-depression with increased State-Trait Anxiety Inventory (STAI) scores [60]. This consequence was not reported in another randomized study [74]. But a recent meta-analysis has shown an association between an increased STAI score and anxiety or depression [75]. A randomized trial reported that students exposed to unexpected simulated patient death had more negative emotions, higher cognitive load, and were less competent to diagnose and manage a case [76]. This risk of negative impact is important to note as an element that could threaten the principle of non-maleficence. There is therefore a dilemma between the principle of beneficence and that of non-maleficence.
In the context of death during SBE, the principle of autonomy involves fully informing learners about the possibility of death and obtaining learners' consent [42]. In one study learners had the same sense of self-efficacy having been informed or not of the possible manikin's death beforehand [77]. The unexpected death of the manikin in simulation is only conceivable and ethical if learners are informed during the pre-briefing and that they give their consent [43, 78].
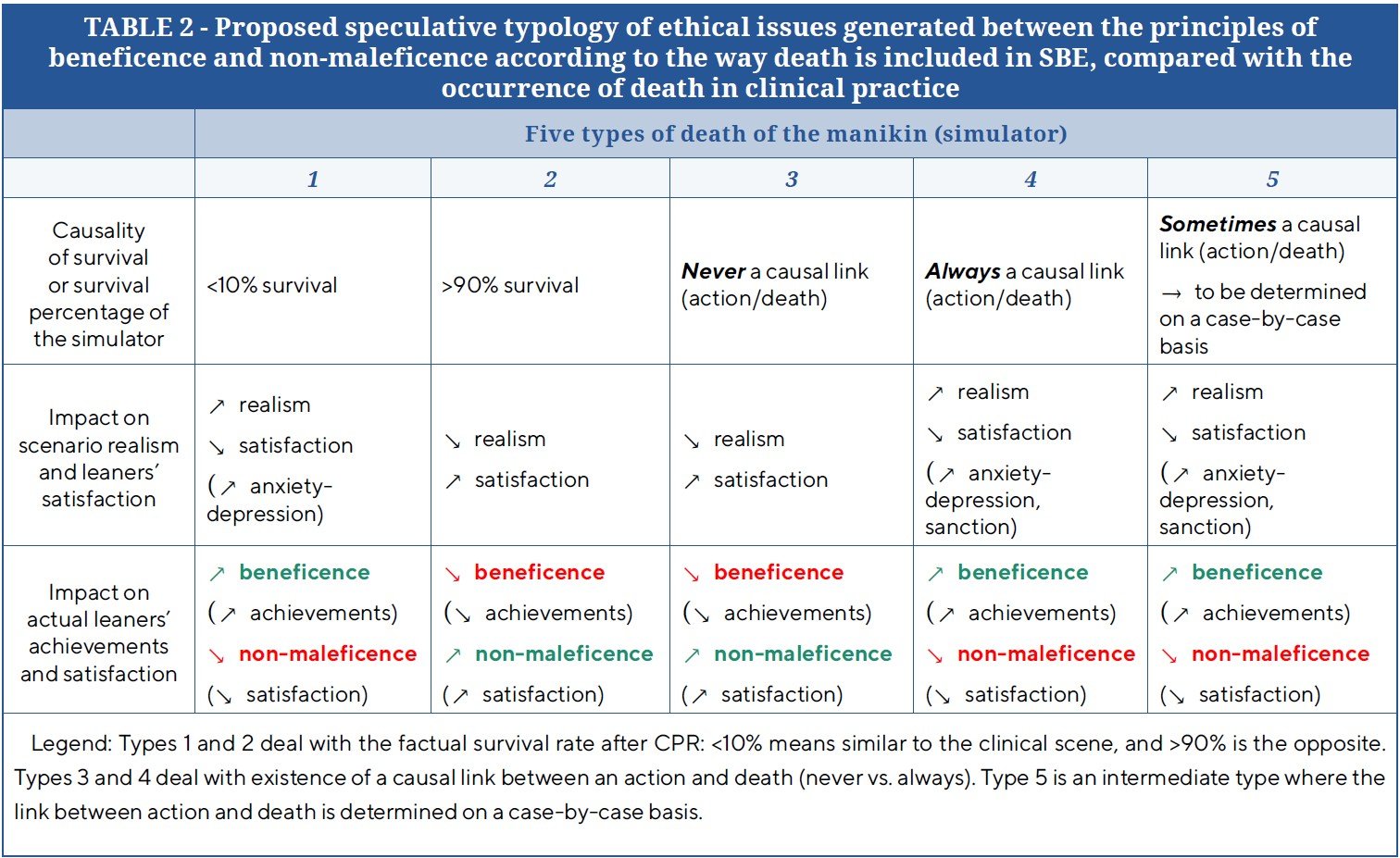
Thus, the possibility of the manikin's death in simulation appears ethical if: 1/ it is appropriate to the scenario; 2/ the learner is experienced and has already seen deteriorating patients; in another words, it should not be with novice learners, given the potentially deleterious effect of the emotional shock of being confronted with death early on in vocational training. [79]; 3/ the principle of autonomy is respected (learners are fully informed beforehand that the manikin may sometimes die) and learners give their consent. Prior to a particularly difficult scenario, it is important to inform learners that it involves 'critical' actions with a strong correlation with whether or not the manikin will survive (Table 2, Type 5).
Table 2 presents different speculative possibilities in relation to the patient’s death during SBE activities. The first possibility is to mimic clinical reality with less than 10% of survival (and increase learning gains and therefore beneficence), but at the risk of learner dissatisfaction and therefore less non-maleficence. Conversely, the second option provides over 90% survival after simulated cardiac arrest, which increases learner satisfaction, but at the risk of being less realistic.
The same applies to option 3 with the manikin surviving all the deleterious learners’ actions that could lead to death. On the other hand, the fourth possibility, which links each deleterious action to the manikin's death, although realistic, seems excessive and will greatly diminish learners' sense of satisfaction.
The fifth possibility of presenting death in simulation seems ethically the least unfavourable. It allows the manikin to sometimes die in very specific cases where the action/inaction of the learners has a strong causal link with the outcome. It is therefore directed by the learners' performance and leads us to consider that a simulation educator may sometimes intentionally deceive learners for their own good (by authorizing the manikin's death if the action with a strong correlation with survival has not been carried out or if inaction is automatically linked to death). This way of representing death in simulation may, in some cases, reduce learner satisfaction and create a degree of frustration, but it also increases learning [43].
Interestingly, this ethical resolution of the problem of death in simulation upsets Kirkpatrick's pyramid at its base, as far as it is not necessary to have learner satisfaction to improve their knowledge or skills. Further research is needed to fully explore this theme, and in particular, the psychological effects of manikin death.
Ethics and research
For the researcher, professional ethics include compliance with the Simulationist Code of Ethics [32, 37], the use of simulation according to one of the 4 modalities described (intervention, evaluation, context, pretext), and full information for the research participant on the same elements as the learner during a simulation session (Pre-briefing and briefing) [80].
When a participant is included in a simulation-based research study, written consent is mandatory [81]. Often there are inconveniences associated with research evaluation studies such as biological sample testing (e.g. blood, urine, saliva), wearing sensors, completing numerous questionnaires, not smoking for 24 hours, etc [82]. To respect the principle of beneficence for all, researchers must provide an equal training opportunity to the “non-simulation” group (control group) participants after the research has been conducted [83].
Ethics and the use of biological tissue
The ethical aim here is not the professional protection of the learner (guaranteed by the educator), but rather the respect and protection of the biological tissue(s) used in the course of a mostly procedural simulation-based activity.
For the educator, it is in all cases a professional ethics of respect for regulations concerning the use of animals or parts of animals [52, 53], and cadavers donated to science [5, 53] as presented in the first example of the foreword. The ethical guarantor with regards to biological tissues is the anatomy laboratory’s ethics committee acting as a protector of the ethics linked to the management of biological tissues [5]. However, the guarantor of ethics with regards to learners remains the educator, responsible for the application of learning regulations (see “Ethics for the learner” above). This dual ethical protection is specific to procedural simulation and must be precisely organized and validated in every SBE activity of this type.
As far as the whole animal is concerned, the essential ethical aspect is to provide sufficient analgesia or anaesthesia so as not to cause suffering [52, 53]. The French National Committee for Ethical Reflection on Animal Experimentation is tasked with ethical issues related to animal experimentation [84].
Concerning the use of cadavers in simulation (complete subjects or anatomical parts), the framework has been precisely defined by a recent French Decree [5], which sets out the principles and procedures (ethics, scientific, and educational committee).
In addition to the guarantees provided by the various committees of the body donation centres (ethical, scientific, and pedagogical) of the Law [5], one must adhere to the respect due to the deceased human body [85], and provide a prevention of viral infections by searching for any viral infectious agents on bodies donated to science before they are used [86].
Teaching ethics through simulation
Learning ethics through simulation plays an important professional role. It contributes to the preservation of values and cultural heritage of societies and healthcare systems, which is a major concern of educational systems [87]. Although not frequently used, simulation enables learners to acquire bioethical principles for the patient [88]. Ethics in medicine and nursing takes place in situations that are inherently uncertain and open-ended [89]. Simulation can be designed to reflect the choices faced by patients and clinicians, and the factors that influence the dynamics between them, and present them in a context that emphasizes the need for a nuanced approach to ethics education and practice [89]. Simulation then provides learners with the opportunity to develop the knowledge and skills needed to manage complex situations and ethical dilemmas [90]. Nevertheless, the complex nature of the scenarios means that they are aimed at end-of-course learners who have already a wide experience of medico-technical situations.
The teaching of bioethics in simulation has been reported in medical [91], nursing [92] and midwifery studies [90]. It is fundamental to teach about ethics in nursing education as nurses are considered the biggest human capital in the health care system [93]. In addition, simulation has been used to determine, on an assessment scale, the threshold value of skills needed in ethical decision-making [94]. Finally, SBE provides insights into the application of bioethics in other countries and cultures [95].
Ethics and computer simulation
According to Moor's Law, there is a correlation between technological advances and social and ethical impacts [96]. VR, and more broadly the sensory virtualization of all or part of the simulation environment, opens up a new dimension of ethical concerns. This development threatens virtue ethics like any new development in human activity [34].
While the potential benefits of VR are heralded by some as limitless possibilities (Metaverse), there is in fact a necessary debate on its real educational efficiency and on the ethical implications that this technology represents in relation to its physiological, cognitive, and behavioural impacts. There may be visual or even pluri-sensory isolation of the educator/learner pair, as well as isolation regarding social dynamics and inter-individual relations [97]. The beneficence of this approach was the first to be raised as potentially threatened or modified by VR for clinicians and patients [98], as well as lay people [99].
The second concern has been distributive justice as simulation using VR is not financially accessible to all training programmes, even though it promises to be an important teaching tool [100]. It seems that currently the crucial problem is that of “virtual ownership” of both the educational content and the information gathered and processed through machine learning. This is a threat to the principle of learner autonomy. For example, a user may be considered the owner of an island in a virtual world, but the entire world, including the island, may be the property of the company that created it and allows users to ”live” in it [101]. For example, the development of many surgical training software is in fact financed by industry, such as implant manufacturers, with the aim not only of promoting the implantation technique for the trained professional, but also of commercially seeding their product to inexperienced learners. A whole virtual economy can develop here, as in Second Life [102].
VR presents a major potential ethical problem, as the technology and financing it imposes can generate a deleterious relationship of dependency between the financial world and the world of healthcare training, particularly through the exploitation of personal physical and psychological data, which may be collected without the knowledge of their authors and for unknown purposes. There is therefore a great vulnerability to this technique, which can be a source of abuse for malicious or financial purposes [103]. The same applies to augmented reality (AR), which can fall victim to misuse and whose data can also be the source of abuse [104]. In order to respect the integrity of human beings and their ability to decide for themselves what is done with their own data, it is essential to lay down precise operating rules for the collection and use of such data [105]. As technology and SBE practices evolve, it is necessary to ensure that ethical principles are always followed, especially as AI may easily ignore related core principles without us realising it. There lay further important ethical questions.
Conclusion
Bioethics was mainly developed for healthcare research and has been extended to patient care. We think it is mandatory to spread its principles to SBE activities with respects to all stakeholders, including the learners, educators, simulated participants, and the patients themselves. Healthcare SBE retains its core ethical foundation of beneficence: “Never the first time on the patient”. However, in its many developments and modalities, simulation must respect bioethical principles. This ethical perspective enables SBE to be seen in a different light and to meet requirements other than those hitherto accepted.
This allows us to explore the ethical dimensions of each stakeholder’s practices in SBE and to see how changes over time can alter ethical tensions, prompting us to exercise greater caution. It also enables the development in each centre, of an SBE network built in accordance with bioethical principles, with the ultimate goal of improving patient care. Research is needed to develop a differentiated perspective based on cultures and practices, in order to better understand the specific characteristics of each.
Author contributions
All authors contributed equally and validated the final version of record.
Declarations
Conflicts Of Interests
The Author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Registration
No registration applicable.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
Ethical approval for this study was not required.
References
1. Smith WR, Audi R. Religious Accommodation in Bioethics and the Practice of Medicine. The J Med Philo. 2021;46(2):188–218. https://doi.org/10.1093/jmp/jhaa038
2. Gray B. (Bio)Ethics in a Pluralistic Society. Challenges. 2019;10(1):12. https://doi.org/10.3390/challe10010012
3. French National Assembly and Senate. Loi 94-654 du 29 juillet 1994 relative au don et à l’utilisation des éléments et produits du corps humain, à l’assistance médicale à la procréation et au diagnostic prénatal [Internet]. Jul 29, 1994. Available from: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000000549618
4. Jouan A. Don de corps à la science : un charnier au coeur de Paris. L’Express [Internet]. 2019 Nov 26; Available from: https://www.lexpress.fr/sciences-sante/sciences/don-de-corps-a-la-science-un-charnier-au-coeur-de-paris_2108389.html?cmp_redirect=true
5. Décret n° 2022-719 du 27 avril 2022 relatif au don de corps à des fins d’enseignement médical et de recherche [Internet]. Apr 27, 2022. Available from: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000045684251
6. Moutel G, Gouriot M, Suzat B, Batteur A, Ploteau S, Destrieux C et al. Don du corps à la science. Med Sci (Paris). 2023;39(2):164–9. https://doi.org/10.1051/medsci/2023011
7. Schicktanz S, Welsch J, Schweda M, Hein A, Rieger JW, Kirste T. AI-assisted ethics? considerations of AI simulation for the ethical assessment and design of assistive technologies. Front Genet. 2023;14:1039839. https://doi.org/10.3389/fgene.2023.1039839
8. Haute Autorité de Santé [Internet]. 2024 [cited 2025 May 22]. Bonnes pratiques en matière de simulation en santé. Available from: https://www.has-sante.fr/jcms/p_3505883/fr/bonnes-pratiques-en-matiere-de-simulation-en-sante
.9. Cook DA, Hatala R, Brydges R, Zendejas B, Szostek JH, Wang AT et al. Technology-Enhanced Simulation for Health Professions Education. JAMA. 2011;306(9):978–88. https://doi.org/10.1001/jama.2011.1234
10. McGaghie WC, Issenberg SB, Cohen MER, Barsuk JH, Wayne DB. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med. 2011;86(6):706–11. https://doi.org/10.1097/acm.0b013e318217e119
11. Beauchamp T, Childress J. Principles of Biomedical Ethics: Marking Its Fortieth Anniversary. The Am J Bioeth. 2019;19(11):9–12. https://doi.org/10.1080/15265161.2019.1665402
12. Ziv A, Wolpe PR, Small SD, Glick S. Simulation-based medical education: an ethical imperative. Acad Med. 2003;78(8):783–8. https://doi.org/10.1097/00001888-200308000-00006
13. Smith A, Lammers S. The ethics of simulation. In: Palaganas JC, Maxworthy JC, Epps CA, Mancini ME, editors. Defining excellence in simulation programs. Philadelphia: Wolters Kluwer; 2014. p. 592–6.
14. Budić I, Pavlović S, Stević M, Petrov I, Perić V, Jović M et al. Medical simulation: Moral and ethical issues. Acta Medica Medianae. 2018;57(1):64–9. https://doi.org/10.5633/amm.2018.0110
15. Garbayo L, Stahl J. Simulation as an ethical imperative and epistemic responsibility for the implementation of medical guidelines in health care. Med Health Care and Philos. 2017;20(1):37–42. https://doi.org/10.1007/s11019-016-9719-0
16. Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a safer health system [Internet]. Kohn LT, Corrigan JM, Donaldson MS, editors. Washington (DC): National Academies Press (US); 2000.
17. French National Assembly and Senate. Loi n° 2002-303 du 4 mars 2002 relative aux droits des malades et à la qualité du système de santé [Internet]. Mar 4, 2002. Available from: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000000227015
18. Graber MA, Wyatt C, Kasparek L, Xu Y. Does Simulator Training for Medical Students Change Patient Opinions and Attitudes toward Medical Student Procedures in the Emergency Department? Acad Emerg Med. 2005;12(7):635–9. https://doi.org/10.1197/j.aem.2005.01.009
19. Kirkpatrick DL. Evaluation of training. In: Donald L, Craig RL, Bittel LR, editors. Training and Development Handbook. New York: McGraw Hill; 1970. p. 87–112.
20. Barsuk JH, McGaghie WC, Cohen ER, O'Leary KJ, Wayne DB. Simulation-based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit. Crit Care Med. 2009;37(10):2697–701.
21. Draycott T, Sibanda T, Owen L, Akande V, Winter C, Reading S et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–82. https://doi.org/10.1111/j.1471-0528.2006.00800.x
22. Cohen ER, Feinglass J, Barsuk JH, Barnard C, O'Donnell A, McGaghie WC et al. Cost savings from reduced catheter-related bloodstream infection after simulation-based education for residents in a medical intensive care unit. Simul Healthc. 2010;5(2):98–102. https://doi.org/10.1097/sih.0b013e3181bc8304
23. Cuvelier L. “Never the first time on a patient”: the stakes of high-fidelity simulation for safety training. Development and Learning in Organizations. 2018;32(5):23–5. https://doi.org/10.1108/DLO-09-2018-131
24. Hssain I, Alinier G, Souaiby N. In-situ simulation: A different approach to patient safety through immersive training. Mediterranean Journal of Emergency Medicine. 2013;15:17–28.
25. Cant RP, Cooper SJ, Lam LL. Hospital nurses' simulation-based education regarding patient safety: A scoping review. Clin Simul Nurs. 2020;44:19–34. https://doi.org/10.1016/j.ecns.2019.11.006
26. McLeod J, McLeod S. Simulation in the Service of Society. SIMULATION. 1988;51(3):130–2. https://doi.org/10.1177/003754978805100307
27. Alinier G, Platt A. International overview of high-level simulation education initiatives in relation to critical care. Nurs Crit Care. 2014;19(1):42–9. https://doi.org/10.1111/nicc.12030
28. Chimbe Phiri E, Chaputula B, Shawa E, Chiaravalli J, Sigalet E, Gabriel J et al. A Simulation Scenario Focused on Resuscitation of a Young Infant (Neonate) for Nurses and Midwives in Malawi, a Limited Resource Country. Cureus. 2018;10(5):e2673. https://doi.org/10.7759/cureus.2673
29. Versantvoort JMD, Kleinhout MY, Ockhuijsen HDL, Bloemenkamp K, de Vries WB, van den Hoogen A. Helping Babies Breathe and its effects on intrapartum-related stillbirths and neonatal mortality in low-resource settings: a systematic review. Arch Dis Child. 2020;105(2):127–33. https://doi.org/10.1136/archdischild-2018-316319
30. Danion J, Breque C, Oriot D, Faure J, Richer J. SimLife® technology in surgical training–a dynamic simulation model. J Visc Surg. 2020;157(3):S117–S22. https://doi.org/10.1016/j.jviscsurg.2020.02.013
31. Haute Autorité de Santé [Internet]. 2012 [cited 2013 January 5] Guide de bonnes pratiques en matière de simulation en santé. Available from: http://www.has-sante.fr/portail/jcms/c_1355008/guide-bonnes-pratiques-simulation-sante-guide
32. Society for Simulation in Healthcare. Simulationist Code of Ethics [Internet]. 2019 [cited 2025 May 22]. Available from: https://www.ssih.org/SSH-Resources/Code-of-Ethics
33. Oriot D, Alinier G. La simulation en santé - Le débriefing clés en mains [Internet]. Masson; 2019. 192 p.
34. Doukas DJ, Ozar DT, Darragh M, de Groot JM, Carter BS, Stout N. Virtue and care ethics & humanism in medical education: a scoping review. BMC Med Educ. 2022;22(1):131. https://doi.org/10.1186/s12909-021-03051-6
35. Ören T. Responsibility, ethics and simulation. Transactions of the Society for Computer Simulation International. 2000;17(4):165–70.
36. Der Sahakian G, Buléon C, Alinier G. Chapter 14 – Educational Foundations of Instructional Design Applied to Simulation-Based Education. In: Chiniara G, editor. Clinical Simulation (Second Edition) [Internet]. Academic Press; 2019. p. 185–206. https://doi.org/10.1016/B978-0-12-815657-5.00014-0
37. Watts PI, Rossler K, Bowler F, Miller C, Charnetski M, Decker S et al. Onward and Upward: Introducing the Healthcare Simulation Standards of Best PracticeTM. Clin Simul Nurs. 2021;58:1–4. https://doi.org/10.1016/j.ecns.2021.08.006
38. Somerville SG, Harrison NM, Lewis SA. Twelve tips for the pre-brief to promote psychological safety in simulation-based education. Med Teach. 2023;45(12):1349–56. https://doi.org/10.1080/0142159x.2023.2214305
39. McDermott DS, Ludlow J, Horsley E, Meakim C. Healthcare Simulation Standards of Best PracticeTM. Prebriefing: Preparation and Briefing. Clin Simul Nurs. 2021;58:9–13. https://doi.org/10.1016/j.ecns.2021.08.008
40. Oriot D, Alinier G. Pocket Book for Simulation Debriefing in Healthcare. Springer; 2018.
41. Der Sahakian G, Alinier G, Savoldelli G, Oriot D, Jaffrelot M, Lecomte F. Setting Conditions for Productive Debriefing. Simulation & Gaming. 2015;46(2):197–208. https://doi.org/10.1177/1046878115576105
42. Alinier G. Developing High-Fidelity Health Care Simulation Scenarios: A Guide for Educators and Professionals. Simulation & Gaming. 2011;42(1):9–26. https://doi.org/10.1177/1046878109355683.
43. Alinier G, Oriot D. Simulation-based education: deceiving learners with good intent. Adv Simul. 2022;7(1):8. https://doi.org/10.1186/s41077-022-00206-3
44. Muckler VC. Exploring Suspension of Disbelief During Simulation-Based Learning. Clin Simul Nurs. 2017;13(1):3–9. https://doi.org/10.1016/j.ecns.2016.09.004
45. Sharma H, Patil AD, Baviskar A. Fiction contract: Its importance in simulation-based medical education. Int J Basic Clin Pharmacol. 2023;12(5):766–70. https://doi.org/10.18203/2319-2003.ijbcp20232579
46. Dieckmann P, Manser T, Wehner T, Rall M. Reality and Fiction Cues in Medical Patient Simulation: An Interview Study with Anesthesiologists. Journal of Cognitive Engineering and Decision Making. 2007;1(2):148–68. https://doi.org/10.1518/155534307X232820
47. Stephan JC, Kanbar A, Saleh N, Alinier G. The effect of deception in simulation-based education in healthcare: a systematic review and meta-analysis. Int J Healthc Simul. 2023:1–14. https://doi.org/10.54531/hwxl4351
48. French National Assembly and Senate. Loi n° 93-121 du 27 janvier 1993 portant diverses mesures d'ordre social [Internet]. Jan 27, 1993. Available from: https://www.legifrance.gouv.fr/loda/id/JORFTEXT000000711603/
49. Direction générale de l’offre de soins; Direction générale de la concurrence de la consommation et de la répression des fraudes. NOTE D’INFORMATION N° DGOS/RH2/2020/157 du 11 septembre 2020 relative à l’application de l’article L. 1453-3 du code de la santé publique aux fins de mise en œuvre du dispositif « encadrement des avantages ». [Internet]. 2020 [cited 2025 Jun 3]. Available from: https://www.economie.gouv.fr/files/files/directions_services/dgccrf/boccrf/2020/20_11/note-d-information-11-septembre-2020.pdf
50. Conférence des Doyens des facultés de Médecine. Charte de la faculté de médecine/santé [Internet]. 2023 [cited 2025 Jun 1]. Available from: https://conferencedesdoyensdemedecine.org/ethique-et-deontologie/
51. Curry AE, Peek-Asa C, Hamann CJ, Mirman JH. Effectiveness of parent-focused interventions to increase teen driver safety: A critical review. Journal of Adolesc Health. 2015;57(1):S6–S14. https://doi.org/10.1016/j.jadohealth.2015.01.003
52. Autissier C. Réglementation éthique de l’expérimentation animale en recherche biomédicale. Médecine/Sciences. 2008;24(4):437–42. https://doi.org/10.1051/medsci/2008244437
53. Rubeis G, Steger F. Is Live-Tissue Training Ethically Justified? An Evidence-based Ethical Analysis. Altern Lab Anim. 2018;46(2):65–71. https://doi.org/10.1177/026119291804600206
54. SoFraSimS. Évaluation Sommative et Simulation en Santé [Internet]. 2022 [cited 2025 May 22]. Available from: https://www.sofrasims.org/articles/117715-evaluation-sommative
55. Alinier G, Shehatta AL, Makker R. Simulation for Clinical Skills in Healthcare Education. In: Nestel D, Reedy G, McKenna L, Gough S, editors. Clinical Education for the Health Professions: Theory and Practice. Singapore: Springer Singapore; 2020. p. 1–21.
56. Alinier G. A typology of educationally focused medical simulation tools. Med Teach. 2007;29(8):e243–50. https://doi.org/10.1080/01421590701551185
57. Kardong-Edgren SS, Farra SL, Alinier G, Young HM. A call to unify definitions of virtual reality. Clin Simul Nurs. 2019;31:28–34. https://doi.org/10.1016/J.ECNS.2019.02.006
58. Sinthuraj V, Makker R, Alinier G. Exploring the benefits, challenges, and psychological safety of using cadaveric simulation in medical education and training. Journal of Emergency Medicine, Trauma, and Acute Care. 2025(2025). https://doi.org/10.5339/jemtac.2025.24
59. Alinier G, Heinrichs W. Chapter 56 – Train-the-Trainers: Creating Simulation Educators. In: Chiniara G, editor. Clinical Simulation (Second Edition) [Internet]. Academic Press; 2019. p. 857–64.
60. Goldberg A, Samuelson S, Khelemsky Y, Katz D, Weinberg A, Levine A et al. Exposure to Simulated Mortality Affects Resident Performance During Assessment Scenarios. Simul Healthc. 2017;12(5):282–8. https://doi.org/10.1097/sih.0000000000000257
61. Calhoun AW, Pian-Smith M, Shah A, Levine A, Gaba D, DeMaria S et al. Guidelines for the Responsible Use of Deception in Simulation: Ethical and Educational Considerations. Simul Healthc. 2020;15(4):282–8. https://doi.org/10.1097/sih.0000000000000440
62. Lewis KL, Bohnert CA, Gammon WL, Hölzer H, Lyman L, Smith C et al. The Association of Standardized Patient Educators (ASPE) Standards of Best Practice (SOBP). Adv Simul (Lond). 2017;2(1):10. https://doi.org/10.1186/s41077-017-0043-4
63. Hendrickx K, Benedicte DW, Wiebren T, Dirk A, Griet P, Wyndaele J-J. Learning intimate examinations with simulated patients: The evaluation of medical students’ performance. Med Teach. 2009;31(4):e139–e47. https://doi.org/10.1080/01421590802516715
64. Maguire P, Faulkner A, Booth K, Elliott C, Hillier V. Helping cancer patients disclose their concerns. Eur J Cancer. 1996;32(1):78–81. https://doi.org/10.1016/0959-8049(95)00527-7
65. Haute Autorité de Santé [Internet]. 2019 [cited 2025 May 22]. Simulation en santé et gestion des risques: Guide méthodologique. Available from: https://www.has-sante.fr/upload/docs/application/pdf/2019-02/guide_methodologique_simulation_en_sante_et_gestion_des_risques.pdf
66. Alinier N, Alinier G. Standardization and professionalization of simulated and standardized patient-based education in Qatar: A call for action. Qatar Med J. 2025;2025(2). https://doi.org/10.5339/qmj.2025.33
67. Al Badawi A. Ethical and Educational Perspectives on Involving Children and Adolescents as Simulated Patients in Pediatric Emergency Training. Panorama of Emergency Medicine. 2026;(under review).
68. Haute Autorité de Santé [Internet]. 2008 [cited 2025 May 22]. Annoncer une mauvaise nouvelle. Available from: https://www.has-sante.fr/upload/docs/application/pdf/2008-10/mauvaisenouvelle_vf.pdf
69. Matos FM, Raemer DB. Mixed-Realism Simulation of Adverse Event Disclosure: An Educational Methodology and Assessment Instrument. Simul Healthc. 2013;8(2):84–90. https://doi.org/10.1097/sih.0b013e31827cbb27
70. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist. 2000;5(4):302–11. https://doi.org/10.1634/theoncologist.5-4-302
71. Lüthi FT, Cantin B. Annonce de mauvaises nouvelles: une pointe d'EPICES dans l'apprentissage. Rev Med Suisse. 2011;7:85–7. https://doi.org/10.53738/REVMED.2011.7.277.0085
72. Corvetto MA, Taekman JM. To Die or Not To Die? A Review of Simulated Death. Simul Healthc. 2013;8(1):8–12. https://doi.org/10.1097/sih.0b013e3182689aff
73. Portanova J, Irvine K, Yi JY, Enguidanos S. It isn’t like this on TV: Revisiting CPR survival rates depicted on popular TV shows. Resuscitation. 2015;96:148–50. https://doi.org/10.1016/j.resuscitation.2015.08.002
74. Philippon AL, Bokobza J, Bloom B, Hurbault A, Duguet A, Riou B et al. Effect of simulated patient death on emergency worker’s anxiety: a cluster randomized trial. Ann Intensive Care. 2016;6(1):60. https://doi.org/10.1186/s13613-016-0163-3
75. Knowles KA, Olatunji BO. Specificity of trait anxiety in anxiety and depression: Meta-analysis of the State-Trait Anxiety Inventory. Clin Psychol Rev. 2020;82:101928. https://doi.org/10.1016/j.cpr.2020.101928
76. Fraser K, Huffman J, Ma I, Sobczak M, McIlwrick J, Wright B et al. The Emotional and Cognitive Impact of Unexpected Simulated Patient Death: A Randomized Controlled Trial. Chest. 2014;145(5):958–63. https://doi.org/10.1378/chest.13-0987
77. Weiss A, Jaffrelot M, Bartier J-C, Pottecher T, Borraccia I, Mahoudeau G et al. Does the unexpected death of the manikin in a simulation maintain the participants’ perceived self-efficacy? An observational prospective study with medical students. BMC Med Educ. 2017;17(1):109. https://doi.org/10.1186/s12909-017-0944-x
78. McIlwaine L, Scarlett V, Venters A, Ker JS. The different levels of learning about dying and death: an evaluation of a personal, professional and interprofessional learning journey. Med Teach. 2007;29(6):e151–e9. https://doi.org/10.1080/01421590701294331
79. Nickerson M, Pollard M. Simulation Philosophy and Practice: Simulator Patient Death Versus Survival. Clin Simul Nurs. 2009;5(3):e147. https://doi.org/10.1016/J.ECNS.2009.04.063
80. Cheng A, Kessler D, Mackinnon R, Chang TP, Nadkarni VM, Hunt EA et al. Reporting guidelines for health care simulation research: extensions to the CONSORT and STROBE statements. Adv Simul (Lond). 2016;1(1):25. https://doi.org/10.1097/sih.0000000000000150
81. Rhodes KV, Miller FG. Simulated Patient Studies: An Ethical Analysis. Milbank Q. 2012;90(4):706–24. https://doi.org/10.1111/j.1468-0009.2012.00680.x
82. Ghazali DA, Ragot S, Breque C, Guechi Y, Boureau-Voultoury A, Petitpas F et al. Randomized controlled trial of multidisciplinary team stress and performance in immersive simulation for management of infant in shock: study protocol. Scand J Trauma Resusc Emerg Med. 2016;24:36. https://doi.org/10.1186/s13049-016-0229-0
83. Alinier G, Hunt B, Gordon R, Harwood C. Effectiveness of intermediate-fidelity simulation training technology in undergraduate nursing education. J Adv Nurs. 2006;54(3):359–69. https://doi.org/10.1111/j.1365-2648.2006.03810.x
84. Ministère de l’éducation nationale, de l’enseignement supérieur et de la recherche. Arrêté du 7 juillet 2006 portant nomination au Comité national de réflexion éthique sur l’expérimentation animale. Journal Officiel, 167 (2006).
85. Touzeil-Divina M, Bouteille-Brigant M. Le droit du défunt. Communications. 2015;97(2):29–43. https://doi.org/10.3917/commu.097.0029
86. Delpech PO, Danion J, Oriot D, Richer JP, Breque C, Faure JP. SimLife a new model of simulation using a pulsated revascularized and reventilated cadaver for surgical education. J Visc Surg. 2017;154(1):15–20. https://doi.org/10.1016/j.jviscsurg.2016.06.006
87. Pinar G, Abay H, Akalin A. The effect of senario-based simulation training technology on knowledge and skills of maternity nursing students in Turkey. Int J Dev Res. 2016;6(6):8096–101.
88. Smith KV, Witt J, Klaassen J, Zimmerman C, Cheng A-L. High-fidelity simulation and legal/ethical concepts:A transformational learning experience. Nurs Ethics. 2012;19(3):390–8. https://doi.org/10.1177/0969733011423559
89. Wilt KE. Simulation-based learning in healthcare ethics education [Doctoral Thesis]. Duquesne University; 2012.
90. Buxton M, Phillippi JC, Collins MR. Simulation: A New Approach to Teaching Ethics. J Midwifery Womens Health. 2015;60(1):70–4. https://doi.org/10.1111/jmwh.12185
91. Lewis G, McCullough M, Maxwell AP, Gormley GJ. Ethical reasoning through simulation: a phenomenological analysis of student experience. Adv Simul (Lond). 2016;1(1):26. https://doi.org/10.1186/s41077-016-0027-9
92. Honkavuo L. Ethics simulation in nursing education: Nursing students' experiences. Nurs Ethics. 2021;28(7–8):1269–81. https://doi.org/10.1177/0969733021994188
93. Cheraghi R, Valizadeh L, Zamanzadeh V, Hassankhani H, Jafarzadeh A. Clarification of ethical principle of the beneficence in nursing care: an integrative review. BMC Nurs. 2023;22(1):89. https://doi.org/10.1186/s12912-023-01246-4
94. Wasson K, Adams WH, Berkowitz K, Danis M, Derse AR, Kuczewski MG et al. What Is the Minimal Competency for a Clinical Ethics Consult Simulation? Setting a Standard for Use of the Assessing Clinical Ethics Skills (ACES) Tool. AJOB Empir Bioeth. 2019;10(3):164–72. https://doi.org/10.1080/23294515.2019.1634653
95. Asao S, Lewis B, Harrison JD, Glass M, Brock TP, Dandu M et al. Ethics Simulation in Global Health Training (ESIGHT). MedEdPORTAL. 2017;13:10590. https://doi.org/10.15766/mep_2374-8265.10590
96. Moor JH. Why We Need Better Ethics for Emerging Technologies. Ethics Inf Technol. 2005;7(3):111–9. https://doi.org/10.1007/s10676-006-0008-0
97. Kenwright B. Virtual Reality: Ethical Challenges and Dangers [Opinion]. IEEE Technol Soc Mag. 2018;37(4):20–5. https://doi.org/10.1109/MTS.2018.2876104
98. Whalley L. Ethical issues in the application of virtual reality to medicine. Comput Biology Med. 1995;25(2):107–14. https://doi.org/10.1016/0010-4825(95)00008-r
99. Ramirez E, Tan J, Elliott M, Gandhi M, Petronio L, editors. An Ethical Code for Commercial VR/AR Applications. In: Intelligent Technologies for Interactive Entertainment. Cham: Springer International Publishing; 2021. p. 15–24. https://doi.org/10.1007/978-3-030-76426-5_2.
100. Iserson KV. Ethics of Virtual Reality in Medical Education and Licensure. Cambridge Quarterly of Healthcare Ethics. 2018;27(2):326–32. https://doi.org/10.1017/s0963180117000652
101. Brey P. Virtual reality and computer simulation. In: Himma KE, Tavani HT, editors. The handbook of information and computer ethics. New Jersey: Wiley; 2008. p. 361–84.
102. Hulsen T. Applications of the metaverse in medicine and healthcare. Adv Lab Med. 2024;5(2):159–65. https://doi.org/10.1515/almed-2023-0124
103. Spiegel JS. The Ethics of Virtual Reality Technology: Social Hazards and Public Policy Recommendations. Sci Eng Ethics. 2018;24(5):1537–50. https://doi.org/10.1007/s11948-017-9979-y
104. Slater M, Gonzalez-Liencres C, Haggard P, Vinkers C, Gregory-Clarke R, Jelley S et al. The Ethics of Realism in Virtual and Augmented Reality. Front Virtual Real. 2020;1:1. https://doi.org/10.3389/frvir.2020.00001
105. Evans J. The IEEE Global Initiative on Ethics of Extended Reality (XR) Report: Extended Reality (XR) Ethics in Medicine [Internet]. The Institute of Electrical and Electronics Engineers, Inc.; 2022 Feb. Available from: https://standards.ieee.org/wp-content/uploads/2022/02/whitepaper-ethics-in-medicine.pdf